1
India and South Africa proposal for WTO waiver from intellectual property protections
for COVID-19-related medical technologies
Briefing Document
Updated 18 November 2020
Contents
INTRODUCTION ................................................................................................................................................ 1
Q&A ....................................................................................................................................................................... 1
IMPACT OF IP BARRIERS ON ACCESS TO THERAPEUTICS, VACCINES AND DIAGNOSTICS ... 6
THERAPEUTICS ................................................................................................................................................... 6
VACCINES ........................................................................................................................................................... 7
DIAGNOSTICS ..................................................................................................................................................... 7
CASE STUDIES EXAMINING IP BARRIERS IN THE CONTEXT OF COVID-19................................... 8
TESTING KIT REAGENTS ...................................................................................................................................... 8
VENTILATOR VALVES ......................................................................................................................................... 8
N95 RESPIRATORS .............................................................................................................................................. 9
ARTICLE IX WAIVERS................................................................................................................................... 10
INTRODUCTION
In a landmark move, India and South Africa on 2 October asked the World Trade Organization
(WTO) to allow all countries to choose to neither grant nor enforce patents and other intellectual
property (IP) related to COVID-19 drugs, vaccines, diagnostics and other technologies for the
duration of the pandemic, until global herd immunity is achieved.
This briefing document aims to provide further details related to this important development,
including a Q&A; an overview of the impact of IP barriers on access to therapeutics, vaccines and
diagnostics; three case studies examining IP barriers in the context of COVID-19; and examples of
Article IX waivers that have been granted with respect to provisions under the Trade-Related Aspects
of Intellectual Property Rights Agreement (TRIPS) Agreement in the past.
Q&A
What has been proposed?
On 2 October 2020, South Africa and India submitted a joint communication to the TRIPS Council at
the WTO, titled “Waiver from certain provisions of the TRIPS agreement for the prevention,
containment and treatment of COVID-19”.
The proposal requests a waiver to be granted to WTO members so that they do not have to implement,
apply or enforce certain obligations related to COVID-19 products and technologies under Section 1
(copyrights and related rights), 4 (industrial design), 5 (patents) and 7 (protection of undisclosed
information) of Part II of the TRIPS Agreement.
2
The proposed waiver would be applicable only to COVID-19. It does not suggest a waiver from all
TRIPS obligations, nor does it suggest a waiver beyond what is needed for COVID-19 prevention,
containment and treatment.
What would it mean if the waiver was granted?
If the waiver was granted, it would allow countries who are WTO members to choose to neither grant
nor enforce patents and other IP related to all COVID-19 drugs, vaccines, diagnostics, and other
technologies, including masks and ventilators, for the duration of the pandemic. This would provide
countries with the policy space needed to collaborate in research and development (R&D),
manufacturing, scaling up, and supplying COVID-19 tools.
What were the outcomes of the 15-16 October WTO TRIPS Council meeting?
The waiver proposed by South Africa and India was presented and discussed on 16 October at a WTO
TRIPS Council meeting.
i
During the session, Kenya and Eswatini joined South Africa and India to
become official cosponsors to the proposal and nearly 100 countries welcomed and showed support
overall for the waiver, while nine WTO members, including the EU, did not support the proposal.
WTO released a statement summarising the discussions at the 15-16 October TRIPS Council.
List of supporters and opponents of the TRIPS waiver proposal, as of 16 October:
- Cosponsors: Eswatini, India, Kenya, South Africa
- In full support: Argentina, Bangladesh, Egypt, Indonesia, Mali, Mauritius, Mozambique,
Nepal, Nicaragua, Pakistan, Sri Lanka, Tunisia, Venezuela, Holy See, UNAIDS, WHO
- Welcomed and supported the general need for further discussions: Chad (least-developed
countries (LDC) Group), Chile, China, Colombia, Costa Rica, Ecuador, El Salvador, Jamaica
(African, Caribbean and Pacific countries (APC) Group), Nigeria, Philippines, Senegal,
Tanzania (Africa Group), Thailand, Turkey
- Opposed or did not support: Australia, Brazil, Canada, EU, Japan, Norway, Switzerland,
United Kingdom, United States
Multiple intergovernmental and international civil society and other organisations expressed their
support for the TRIPS waiver proposal either during the TRIPS Council meeting or outside of WTO,
including: African Commission of Human and Peoples' Rights, Amnesty International, Drugs for
Neglected Diseases initiative (DNDi), Human Rights Watch, MSF, People’s Health Movement, South
Centre, Third World Network, Joint United Nations Programme on HIV/AIDS (UNAIDS), Unitaid,
Experts of the UN Office of the High Commissioner for Human Rights, and World Health
Organization (WHO). More than 300 civil society organisations globally have called for governments
to support the proposal.
What are the next steps in the process?
Discussions will continue at the upcoming WTO TRIPS Council meetings this year, 20 November
and early December in Geneva.
Between now and the end of the year, South Africa and India are seeking to increase support from
WTO members for the waiver proposal. Following the upcoming sessions of the TRIPS Council, a
report will be submitted to the WTO General Council ahead of a General Council session scheduled
for 16-17 December. It is anticipated that another round of discussions will take place during this 16-
17 December meeting, and the process could potentially continue into 2021.
ii
South Africa’s opening and closing statements can be found here; India’s opening statement can be found here.
3
Is it legal to request a waiver from obligations under the TRIPS Agreement?
Yes. Article IX 3 and 4 of the Marrakesh Agreement Establishing the WTO (WTO Agreement),
affirm that in exceptional circumstances, a waiver from certain obligations under WTO treaties, such
as TRIPS, can be decided at the WTO Ministerial Conference (during the interval of the Conferences,
the WTO General Council would perform this function). The waiver needs to contain a justification
based on the exceptional circumstances, the conditions and the time when the waiver terminates.
Waivers longer than one year will be reviewed by the Ministerial Conference annually until its
termination.
Does the waiver proposed apply only to developing countries?
No. The proposal calls for a waiver to be applicable for all WTO members – including developing,
developed, and least-developed countries (LDCs).
How is a final decision reached at WTO on a waiver?
According to the decision-making rules of WTO (Article IX of WTO Agreement), the application for
a waiver must be submitted to the TRIPS Council first and then decided at the Ministerial Conference
or the General Council.
After receiving the application for a waiver, the TRIPS Council must consider it within 90 days, and
then submit a report to the Ministerial Conference – the highest decision-making body that consists of
all WTO members – for a decision. The Ministerial Conference is held every two years, with the next
one planned for June 2021. In the interim, the General Council of WTO functions on behalf of the
Ministerial Conference (Article IV.2 of the WTO Agreement). In this case, a report will be submitted
to the WTO General Council ahead of a General Council session scheduled for 16-17 December.
The decision to grant the waiver will be reached based on consensus of all WTO members. If
consensus cannot be reached, the decision can be made by voting. A three-fourths majority is needed
for a decision to be made through voting.
Has a consensus been reached by WTO members to grant waivers in the past?
Yes, many waivers have been adopted by WTO members.
For example, in 2003, WTO members reached a consensus for a waiver related to Paragraph 6 of the
Doha Declaration on the TRIPS Agreement and Public Health. The waiver established a mechanism
to allow countries producing generic medicines under a compulsory license to supply the medicines to
other countries that lacked the manufacturing capacity required to produce the medicines themselves.
Transition periods and waivers granted to least-developed countries (LDCs):
LDCs enjoy special exemptions from implementation of the TRIPS Agreement under Article 66.1 of
the Agreement. LDC members do not have to implement any aspect of the TRIPS Agreement (other
than Articles 3, 4 and 5) until July 2021. As this transition period is coming to an end, the LDC Group
in WTO has submitted a request to extend the period for as long as a country remains an LDC, plus an
additional period of 12 years once they graduate from the LDC status. This request (IP/C/W/668) was
discussed at the 15-16 October TRIPS Council meeting and will be discussed at subsequent sessions.
The request should be supported by all members.
In addition, more specifically with respect to pharmaceutical products, LDCs do not have to
implement, apply or enforce Section 5 (on patents) and Section 7 (on protection of undisclosed
information) of TRIPS until 1 January 2033. Linked to this decision, LDCs have been granted waivers
under Article IX of the WTO Agreement from obligations pertaining to exclusive marketing rights
and mailbox obligations (Article 70.8 and 70.9 of TRIPS Agreement).

4
Is the waiver permanent?
The proposal submitted by South Africa and India suggests that the waiver should remain valid until
the majority of the world’s population has access to effective vaccines and has developed immunity to
COVID-19. The actual duration of the waiver is unknown, but it will depend on negotiations by
members and is time-limited based on WTO rules.
Why is the waiver important at this moment in the pandemic?
All governments are facing challenges ensuring timely, sufficient and affordable access to effective
medicines, vaccines, diagnostics and other essential medical tools. This is especially challenging,
however, for many developing countries that face limitations developing and scaling up
manufacturing capacity due to IP barriers. The unprecedented situation today requires that all IP,
knowledge, technology and data related to COVID-19 health technologies can be utilised by everyone
to ensure uninterrupted production and supply by any competent country or manufacturer worldwide.
To achieve this, governments have a collective responsibility to address IP and technology barriers.
Since the start of this pandemic, pharmaceutical corporations have continued with their ‘business-as-
usual’ approaches either by maintaining rigid control over their proprietary IP rights or by pursuing
secretive and monopolistic commercial deals and excluding countries heavily affected by COVID-19.
The pharmaceutical industry as a whole has also chosen not to engage with the WHO COVID-19
Technology Access Pool (C-TAP) initiative that aims to encourage the voluntary contribution of IP,
technologies and data to support global sharing and scale-up of manufacturing and supply of COVID-
19 health technologies.
Despite having received at least US$70.5 million of public funding to develop remdesivir, one of the
candidate drugs for COVID-19 treatment, pharmaceutical corporation Gilead has signed secretive
bilateral deals with a few generic companies of its choosing that exclude nearly half of the world’s
population from its licensed territories.
These recent actions by pharmaceutical corporations show that relying on their exclusive rights and
limited voluntary actions is not the solution in a global pandemic. Governments need to be in the
driver’s seat and fulfil their core obligations of protecting public health and ensuring access to
medicines for all. The waiver proposal by India and South Africa presents an important opportunity
for all governments to unite and stand up for public health, global solidarity, and equitable access
through a concrete step at the international level that can provide an automatic and expedited solution
to address IP and technology challenges collectively.
How do we know that overcoming intellectual property monopolies can help increase access to
medical tools? What can we learn from past?
Twenty years ago, the price charged for the triple cocktail of drugs to treat HIV was over $10,000 for
one person for one year, because of patent monopolies. People across the world were left to die
because they could not afford the deliberately high prices companies charged for these medicines. In
South Africa and other countries around the world, an emerging access-to-medicines movement
including patient activists, civil society and health-rights groups, stood up to the pharmaceutical
industry and government inaction to get HIV medicines to the people who needed them to survive. It
worked. By overcoming the companies’ monopolies on these drugs and fostering generic production
and competition, the price of antiretroviral drugs dropped 99% over the next decade, paving the way
towards scaling up treatment for people living with HIV to over 25 million in 2019.
The situation today with the COVID-19 pandemic is similar. As countries scramble to ensure access
to the medical tools they need to respond to the pandemic, we are seeing business-as-usual approaches
from the pharmaceutical industry. If the TRIPS waiver proposal is approved, it could signal a major
turning point in countries’ response to the COVID-19 pandemic, ushering in a much-needed wave of
access to COVID-19 medical tools and technologies.
5
Some people say IP is not an issue for COVID-19 tools. If that is true, why is a waiver needed?
We disagree with this claim. Both past experiences and current actions have shown concretely that IP
does pose a challenge in ensuring global equitable access to the effective tools needed in response to
COVID-19, including vaccines.
In the last few months, treatment providers and governments have faced IP barriers
over drugs, masks, ventilator valves and reagents for testing kits. Countries are facing shortages of
remdesivir, which is widely patented but licensed in a manner that allows generic supply only in a
limited number of countries. In addition, multiple patents have been filed for COVID-19 vaccines in
development, for example, more than 100 patents have been filed for the mRNA technology that
Moderna is using to develop a vaccine. Although Moderna recently announced that it would not
enforce its patents during the pandemic – the only vaccine corporation to do this thus far – the
company did so after losing an important patent dispute and failing to disclose the US federal funding
it received in the patent applications for its mRNA vaccine. In addition to following through on its
previous commitment to not enforce its patents, Moderna must share all IP, including the necessary
technology, data and know-how, so that other manufacturers can scale up production of these
potentially lifesaving vaccines. Many COVID-19 vaccine developers, including Pfizer/BioNTech,
have taken no steps towards licensing or transferring IP-protected technologies to enable increased
global manufacturing capacity and supply.
A report by MSF found that patents pose a serious threat to access to affordable versions of newer
vaccines like pneumococcal conjugate vaccines (PCV) and human papillomavirus (HPV) vaccines.
The report provides an overview of the excessive patenting strategy of the vaccine industry and
identifies patents that have been sought throughout the entire process of vaccine development, ranging
from basic research, starting materials, vaccine composition and final products, to the methods of
vaccination, including vaccination schedules. These practices and experiences should not be repeated
in this pandemic as they would delay the availability and universal access to future COVID-19
vaccines.
Why do countries need a waiver when they can already use TRIPS flexibilities for public
health?
The waiver and existing TRIPS flexibilities are not mutually exclusive.
The proposal for a waiver on certain IP provisions offers an expedited, open and automatic global
solution that allows for uninterrupted collaboration in development and scale-up of production and
supply and that collectively addresses the global challenge facing all countries.
Countries should continue to use TRIPS flexibilities to safeguard public health, including issuing
compulsory licenses and placing limitations on or making exceptions to exclusive rights. However,
the “case by case” or “product by product” approach required when using flexibilities to address IP
barriers at the national level could be limiting during the pandemic. Some countries also face
limitations with respect to their national laws, face pressures from their trading partners, or lack the
practical and institutional capacity required to exercise TRIPS flexibilities during the pandemic
quickly and effectively.
Given these common challenges, and the pharmaceutical industry’s refusal to routinely offer non-
exclusive licenses with worldwide coverage to facilitate global access, it is critical for governments to
address this global crisis as they did nearly 20 years ago under the Doha Declaration on the TRIPS
Agreement and Public Health amidst the HIV/AIDS epidemic and support this landmark move by
India and South Africa.
6
Limitations of relying on a “case by case” and “product by product” approach to address IP
barriers:
1. The development of COVID-19 medicines, vaccines and diagnostics is evolving rapidly,
and it is challenging for countries to select one or two specific products to target.
2. There is a practical need for countries to collaborate and share manufacturing and supply
capacities to achieve a truly global response. When countries lack immediate
manufacturing capacity for any of the essential parts for a product, including raw materials,
components or packaging materials, removing IP barriers on one product in one country
alone will not be sufficient. Other countries who can produce the required materials and
parts need to ensure that they are monopoly free so that they can support other countries by
freely exporting the materials based on need. Likewise, countries who have the capacity to
produce a finished product would need to ensure that there are no restrictions for them to
export the product to any other countries in need. Responding to COVID-19 effectively
requires a collective and global solution that overcomes the restrictions of addressing IP
barriers on a national level so that countries can collaborate and freely share manufacturing
and supply capacities.
3. The existing mechanisms for compulsory licenses under Article 31 and Article 31bis of the
TRIPS Agreement contain territorial and procedural restrictions that make the practice of
issuing product-by-product compulsory licenses a complex process, making it difficult for
countries to collaborate.
a. Article 31 requires that compulsory licenses are issued on a case-by-case basis and
used predominantly to supply domestic markets, thereby limiting the ability of
manufacturing countries to export to countries in need.
b. Article 31bis requires that any product produced and exported under a compulsory
license be identified with specific packaging and quantities, which can lead to
unnecessary delays in the context of COVID-19 where countries need urgent access
to medical tools.
MSF’s experience trying to buy drugs under this mechanism showed that the rules are
prohibitively complex and offer neither an expedited nor global solution.
IMPACT OF IP BARRIERS ON ACCESS TO THERAPEUTICS, VACCINES AND
DIAGNOSTICS
Therapeutics
The example of remdesivir reveals a typical example of how IP barriers affect global access to
COVID-19 therapeutics. The primary patent on the base compound of remdesivir has been granted to
Gilead in more than 70 countries, which means that when countries are not covered by a voluntary
license or do not use other measures to overcome the patents, they may be blocked from getting
access to generic alternatives until 2031. After ignoring demands calling for non-enforcement of its
patents on remdesivir, Gilead proceeded to secretly sign voluntary licensing agreements with only a
few manufacturers of its choosing. The voluntary licensing agreements excluded nearly half of the
world’s population from accessing more affordable generics, including most South American
countries and many countries with manufacturing capacity, some of which have supported COVID-19
related clinical trials. Today many countries are facing shortages of remdesivir in their health systems.
This dangerous precedent set by Gilead must alert governments that voluntary actions of companies
are not reliable.
In addition, there is an emerging cluster of biologic medicine candidates, including a group of
repurposed monoclonal antibodies, such as sarilumab and tocilizumab, and a group of specific new
antiviral monoclonal antibodies that are currently being investigated as potential COVID-19
treatments in clinical trials. Many of these monoclonal antibody candidate therapeutics are still under
7
patent protection in many developing countries such as Brazil, South Africa, India, Indonesia, China
and Malaysia. This means that if some of these therapeutics show clear efficacy, production and
supply by diverse manufacturers in different countries would be challenging unless governments take
early actions to address these barriers. Preliminary patent data shows that primary and secondary
patent applications have been widely filed or granted for some of the antiviral and monoclonal
antibody candidates, such as molnupiravir, AT-527 and baricitinib, including in developing countries.
Vaccines
Since the start of the pandemic, there has been a constant denial or avoidance by some institutions and
lobby groups of the pharmaceutical industry stating that IP is not an issue in the context of addressing
the possible scarcity of vaccine supplies. Such a statement is at odds with what MSF has documented
with other essential vaccines prior to COVID-19, and with what has been observed and analysed
during this pandemic.
In 2017, MSF published a report documenting the effects of patents in hindering the introduction of
affordable vaccines in developing countries, with a focus on pneumococcal conjugate vaccines (PCV)
and the human papillomavirus (HPV) vaccine. The report summarises that patents have been applied
for or granted across the entire process of vaccine development, production and use. Patents were
identified on vaccine-production materials such as chemical reagents, host cells, vectors, and
DNA/RNA sequences; vaccine compositions; process technologies; vaccination age groups; methods
of using vaccines; and vaccine schedules and presentations. These patents increase uncertainty and
costs, delay competition and keep prices high for low- and middle-income countries, hindering
people’s access to important vaccines.
In 2016-2017, MSF filed a patent opposition and later a writ petition to challenge Pfizer’s vaccine
composition patent that has blocked India from developing alternative versions of Pfizer’s PCV13
vaccine. The equivalent patent has been granted in South Korea, which compelled a Korean vaccine
developer to close their development of an alternative PCV13.
In the context of COVID-19, IP barriers have been reported in vaccine patent disputes and can hinder
vaccine development. Research has revealed that a large portfolio of background IP, such as more
than 100 patents on mRNA platform technologies that are used for COVID-19 vaccines, has already
been granted on key technology platforms used for COVID-19 vaccine development. Several bilateral
voluntary agreements have been signed between vaccine developers and producers since the start of
the pandemic on possible vaccine candidates, but most of the agreements have not been made publicly
available to allow for an assessment of the scope and conditions.
While Brazilian public research institution Fundação Oswaldo Cruz (Fiocruz) has taken an important
step to publish the license signed with pharmaceutical corporation AstraZeneca (who acquired IP
rights on the vaccine from the Oxford University), important terms and conditions around the scope of
IP and the right to use have been redacted because of AstraZeneca’s claim for commercial secrecy.
Most of the vaccine companies, including Pfizer and its partner BioNTech, have indicated no plans to
license or transfer their IP-protected technologies to enable increased global manufacturing capacity
and supply. MSF’s past experiences demonstrate clearly that restrictive license terms can have a
detrimental impact on access.
Governments must learn from these past experiences and take the appropriate steps to ensure that
access to new vaccines in developing countries is not compromised or blocked due to IP and
monopolies.
Diagnostics
The lack of access to affordable, adapted and simplified diagnostic tests for infectious diseases such
as tuberculosis (TB), HIV and hepatitis C (HCV) in resource-limited settings has been an ongoing
struggle. Starting in 2017, MSF conducted a series of analyses on the causes of market monopolies in
8
the field of diagnostics for infectious diseases, especially concerning TB, HIV and HCV, and
examined the patent landscape of three point-of-care diagnostics that are important in MSF’s medical
programmes: Xpert MTB/RIF (produced by Cepheid), AlereQ HIV-1/2 Detect (produced by Abbott)
and OraQuick HCV Rapid Antibody Test (produced by OraSure).
MSF’s analysis shows that the overall business model for diagnostics results in multiple dominant
closed diagnostics systems (since each major diagnostics company develops both the device and the
consumable parts – for example, the reagent kits or reagent-loaded integrated cartridges – specifically
tailored to that device), making competition extremely difficult. The high cost and burden of
switching between systems results in a “locked-in” effect for end users since they have no choice but
to buy both the device and the assays from the same company. Although it’s not possible to say that
one or two access-blocking patents are the key barrier, the analysis shows that major diagnostics
companies hold a considerable number of patents, often bundled into thickets for various
instrumentation, assays, methods and software, related to different aspects of the technologies,
methodologies and devices. This proliferation of patents may contribute to discouraging the
development of open platforms for interoperable diagnostics.
CASE STUDIES EXAMINING IP BARRIERS IN THE CONTEXT OF COVID-19
The following three case studies are based on published news reports and were developed with the
support of Third World Network (TWN).
Testing kit reagents
The majority of COVID-19 laboratories in the Netherlands work with equipment made by
pharmaceutical corporation Roche and depend on the company for supplies of the testing reagents,
which are the liquid buffer needed to run the tests. A shortage of this buffer is one of the reasons why
the Netherlands was not able to carry out mass testing for COVID-19 during the early stages of the
pandemic in late March.
Despite the shortage, Roche initially refused to provide the recipe for the buffer, blocking laboratories
from quickly making their own solution and ramping up their testing capability. Following public
pressure, and after the Dutch Health Minister suggested issuing a compulsory license on the buffer
formula, and the European Commission started to investigate Roche for possible abuse of its market
position, Roche agreed to release the buffer recipe for others to make.
IP can pose a barrier to produce testing kit reagents, including tests for COVID-19, which can
negatively impact a laboratory’s or country’s ability to screen samples for COVID-19 – an essential
part of controlling the pandemic. Companies must share the recipes for critical medical products, like
test reagents, to ensure the scale-up of supply worldwide.
Ventilator valves
As reported in March 2020, a northern Italian hospital started to run out of ventilator valves and their
regular supplier was not able to produce more in the short term. Two engineers from a nearby start-up
with a 3D printer offered to help manufacture more valves. After the manufacturer denied access to
the valve’s blueprint and threatened to sue for patent infringement, the engineers proceeded to reverse
engineer a 3D-printed version themselves. The 3D-printed replacement valves, which saved many
lives, cost about $2-3 each to produce, compared to $11,000 per valve from the manufacturer, and can
be manufactured in a fraction of the time. The engineers received hundreds of requests for their 3D-
printed valves, but did not share their digital print file more widely due to possible legal and medical
issues.
9
Following the story, a law firm warned that “[m]anufacturers should be aware of the complex
intellectual property issues concerned with this 3D printing technology. In scanning a component such
as a valve, and manufacturing a part using 3D printing equipment, there is a risk that this action will
infringe an existing patent, design or copyright which protects the component, leading to an injunction
or claim from the rights holder for damages or other remedies (such as delivery up of infringing
parts).”
There are complex legal implications when producing copies of lifesaving medical tools. Any person
or company intending to manufacture parts using 3D printing would have to identify: the extent of IP
protection (including patents or registered design); who are the IP holders; and whether the IP holders
are willing to permit the parts to be manufactured (including the terms and conditions that the right
holder will impose). This is a costly, time-consuming, and complex process as there could be multiple
IP holders, and an IP holder may refuse to license its IP.
In March 2020, WHO noted a shortage of ventilators around the world. Removing IP barriers,
including those around 3D printing, can be critical to address life threatening shortages during this
pandemic.
N95 respirators
N95 respirators, a critical type of protective mask for healthcare workers, has been in short supply
throughout the COVID-19 pandemic. The respirator is protected by hundreds of patents owned by the
US government, the multinational company 3M, paper and healthcare companies, individuals and
universities. In March 2020, the Governor of Kentucky in the United States called on 3M to release its
patent for the N95 respirator so that more manufacturers could start producing it. The company has
not released its patent to date.
IP barriers, including patents, have exacerbated the shortages of N95 respirators faced by hospitals
around the world. Companies and others holding patents on important tools, including masks, should
announce now that they will not enforce their patents so that healthcare workers on the frontline of
this pandemic can be protected.
10
ARTICLE IX WAIVERS
Many Article IX waivers on various trade issues have been granted at the WTO benefiting different
members including developed, developing and least-developed countries (see, for example, the list of
waivers granted 1995-2015 and 2019). Table 1 below presents a non-exhaustive list of Article IX
waivers granted with respect to provisions under the TRIPS Agreement.
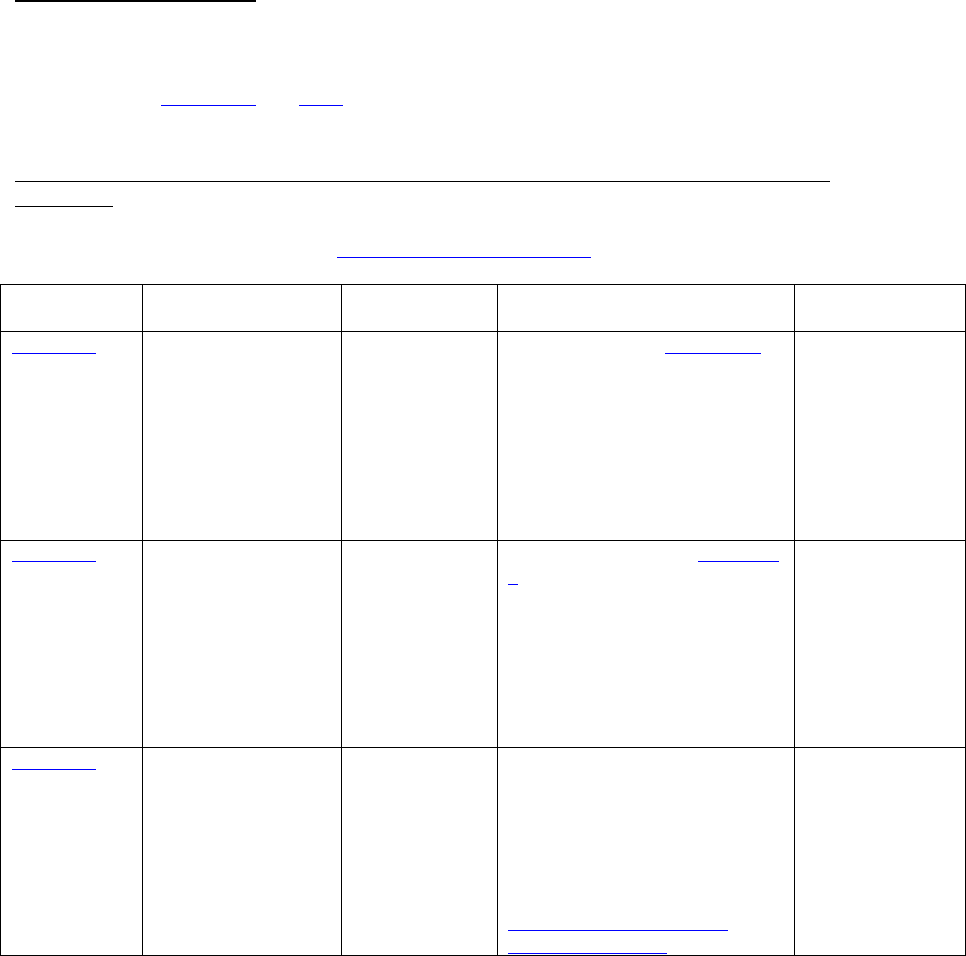
Table 1. Examples of Article IX waivers granted with respect to provisions under the TRIPS
Agreement
Table developed with the support of Third World Network (TWN)
Decision
number
Provisions waived
Beneficiaries
Grounds of the waiver
Duration
WT/L/478
TRIPS Agreement
Article 70.9 with
respect to
pharmaceutical
products
LDC members
In accordance with Paragraph 7 of
the Doha Declaration on the
TRIPS Agreement and Public
Health, LDC members do not
have to implement, apply or
enforce Section 5 (on patents) and
Section 7 (on protection of
undisclosed information) of the
TRIPS Agreement.
Until 1 January
2016 (about 13
years)
WT/L/540
TRIPS Agreement
Paragraph 6 decision
waiving Paragraphs
(f) and (h) of Article
31
All WTO
members except
those who opted
out
The need to implement Paragraph
6 of the Doha Declaration on the
TRIPS Agreement and Public
Health to find a rapid solution to
help countries with insufficient or
no manufacturing capacities in the
pharmaceutical sector make
effective use of compulsory
licenses.
Until the date on
which an
amendment to the
TRIPS Agreement
replacing its
provisions takes
effect for that
member
WT/L/971
TRIPS Agreement
Article 70.8 and 70.9
with respect to
pharmaceutical
products
LDC members
In line with the waiver decision
WT/L/478, reaffirm that LDC
members do not have to
implement, apply or enforce
obligations under
Article 70.8 and 70.9 of the
TRIPS Agreement with respect to
exclusive market rights and
mailbox obligations.
Until 1 January
2033, or until a
country graduates
from the LDC
status (about 17
years)
